SPAIN FIFTY-FIFTY PROGRAM
“IF ADULTS ARE TRAINED IN PEER GROUPS AND PROVIDED WITH THE KNOWLEDGE, SKILLS AND ATTITUDES A HEALTHY LIFESTYLE REQUIRES, THEIR CARDIOVASCULAR HEALTH HABITS AND THEIR OWN SELF-CONTROL OF THE RISK FACTORS WILL IMPROVE”

The 50/50 (Fifty-Fifty) Programme A randomized, controlled trial evaluating a community intervention in cardiovascular risk factors
Obesity, smoking, a sedentary lifestyle and high blood pressure are the main risk factors for the development of cardiovascular diseases, which in turn are the leading cause of mortality in Spain and in the rest of the world. In Spain the prevalence in adults of overweight is: 36%, obesity: 17%, smoking: 26% and sedentary life: 37%. As a result, the Spanish Agency of Consumer Affairs, Food Security and Nutrition (AESAN) from the Spanish Ministry of Consumer Affairs and the SHE Foundation, promoted the introduction of the Fifty-Fifty Program in 8 Spanish cities and towns. This Program constitutes a community intervention trial designed by Dr. Valentín Fuster with the aim of improving comprehensive health in adults, helping them to establish self-control of the main risk factors for such diseases. The participants in the study were healthy adults between 25-50 years of age and with at least one cardiovascular risk factor who participated in educational and motivational workshops involving peer-assisted learning groups, with the purpose of promoting healthy living habits. After one year of follow-up, 67% of the participants were seen to have improved in relation to the 5 cardiovascular risk factors, and almost one half reduced smoking – thus demonstrating the effectiveness of health promotion through the peer community intervention.




In view of the great increase in the prevalence of cardiovascular diseases, there is an urgent need to adopt multisector strategies focused particularly on primary prevention, through the offering of quality healthcare services that promote a healthy lifestyle and reduce cardiovascular risk factors, mortality and morbidity.
In Spain, cardiovascular diseases are the leading cause of mortality or disability [1]. However, cardiovascular health (as defined by the American Heart Association) in this country is poor, particularly in reference to lifestyle [2]. Less than 1% of all Spaniards reach ideal values for the 7 cardiovascular health indicators and thus have a healthy lifestyle [3]. Furthermore, a full quarter of the population is characterized by a lack of physical exercise, smoking and obesity (Figure 1) [4].
These cardiovascular risk factors, together with high blood pressure, can be reduced through the acquisition of healthy habits and behaviors. Peer support systems have yielded positive results in many chronic illnesses [5]. However, randomized clinical trials are needed to assess the efficacy of this kind of strategy in modifying cardiovascular risk factors.

Based on previous scientific learnings, Dr. Fuster initiated a pilot project in the town of Cardona (Barcelona, Spain). The good results obtained facilitated the conduction of a larger study in another 7 Spanish cities and towns: Barcelona, Cambrils, Guadix, Manresa, Molina de Segura, San Fernando de Henares and Villanueva de la Cañada (Figure 2). This study involved 543 volunteers (71% females), each with at least one cardiovascular risk factor (20% with arterial hypertension (≥ 140/90 mmHg), 82% overweight (body mass index ≥ 25), 81% with a sedentary lifestyle (≤ 150 min. of physical activity a week) and 31% smokers). The Program received the collaboration of the Spanish Federation of Municipalities and Provinces (FEMP), and of the local authorities of the participating cities and towns.

Figure 2. Fifty-Fifty Program: Cities and towns participating in the study.
The intervention was based on elements of Social Cognitive Theory [10]. This theory explains human behavior in terms of a three-dimensional dynamic reciprocity model characterized by the continuous interaction of personal, environmental and behavioral factors. The key elements of this theory include observational learning, reinforcement, self-control and self-efficacy.
In order to promote cardiovascular health, the Program used evidence-based recommendations such as increased physical activity according to the guidelines of the WHO (150 min. a week), improved eating habits in order to comply with the recommendation of 5 portions (400 g) of fruit and vegetables a day, and smoking cessation.
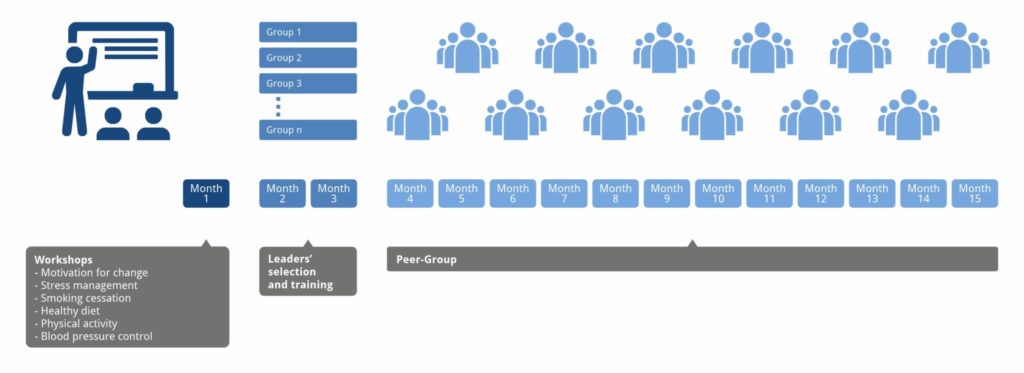
In a first phase lasting two months, all the participants were enrolled in educational and motivational workshops designed to promote healthy living habits. The meetings were used to address motivations for change, coping with stress, smoking cessation, healthy eating habits, regular physical exercise, and blood pressure self-control. Then, in a second phase lasting 12 months, the participants were randomized to two groups (1:1): an intervention group, involving group dynamics educational activities; and a control group, simply subjected to follow-up during the same period of time (Figure 3). The participants in the intervention group were randomized to subgroups with about 10 people each, in which two subjects were chosen as leaders or educators by psychologists and health professionals [11]. All the selected educators attended a three-hour session on health and the promotion of health, leadership and communication skills. Each month, the intervention groups of each city or town held group dynamics sessions lasting 60-90 minutes, based on “peer education” and designed to promote internal changes and offer the participants the possibility of developing skills other than simple knowledge to help control the cardiovascular risk factors. In each intervention group the participants explained the improvements in their healthy habits and the difficulties found. A registry was made of all the data referred to reduction of the cardiovascular risk factors and improvement of healthy habits, with a view to assessing the success of the intervention over the middle and long term [12, 13].
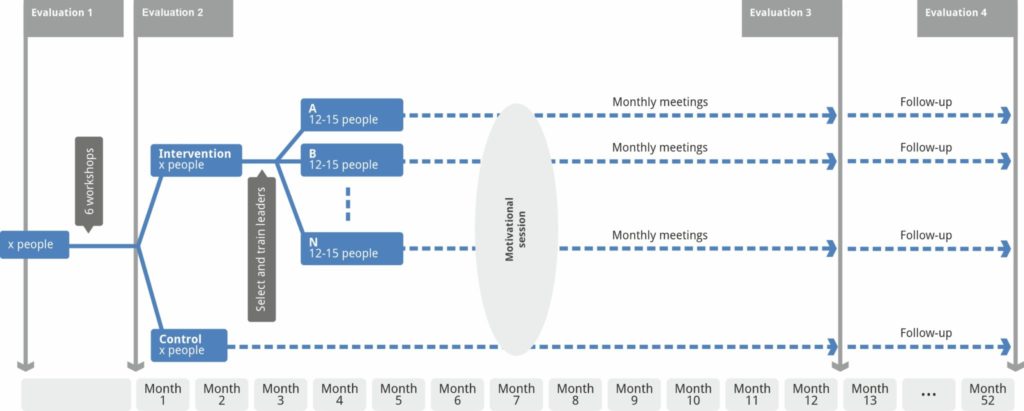
Figure 3. Conceptual map of the Fifty-Fifty Program.
The main outcome assessed by the study was the mean change in a composite score related to blood pressure, exercise, weight, diet and smoking (Fuster-BEWAT score).
A total of 4 assessments were performed: at baseline, after the training workshops, over the 12 months (after the group dynamics), and over the 40 months.
The investigators have performed a new analysis of cardiovascular risk factors 12 months and 40 months after the end of the study to assess the progression of the participants [14]. The results obtained from the Fifty-Fifty study confirm that educating adults in knowledge, skills and attitudes about a healthy lifestyle, accompanied by peer support, improves cardiovascular health habits and self-management of risk factors, and confirms the importance of giving continuity to support dynamics.
The Fifty-Fifty Program has also been applied in Spanish companies with the aim of providing tools to improve the cardiovascular health of their workers. Some of the companies that have applied the program are Port Aventura (theme park) and AMPO (steel foundry). Employees who participated in the various editions of the program showed an overall improvement in the BEWAT score and its individual components, especially in blood pressure, diet and smoking cessation.
It is essential to implement programs to promote healthy habits which, like this one, are of great value in raising public awareness, since, in the words of Dr. Fuster, “we must not prevent disease, we must promote health”.
References
- Banegas JR et al. Rev Esp Cardiol Supl, 2006, 6(G):3-12. Epidemiología de las enfermedades cardiovasculares en España.
- Lloyd-Jones DM et al. Circulation, 2010, 121(4):586-613. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond.
- Graciani A et al. Circ Cardiovasc Qual Outcomes, 2013, 6(1):90-8. Cardiovascular health in a southern Mediterranean European country: a nationwide population-based study.
- Lopez-Garcia E et al. Atherosclerosis, 2013, 231(1):152-7. Prevalence and determinants of metabolically healthy obesity in Spain.
- Funnell MM. Diabetes Self Manag, 2010, 27(5):8, 11-3. Peer support, education, and mentoring.
- Banegas JR et al. Rev Esp Cardiol, 2011, ISSN 0300-8932, 64(10):876-882. Estudio de Nutrición y Riesgo Cardiovascular en España (ENRICA).
- Álvarez E et al. Ministerio de Sanidad, Política Social e Igualdad, 2011. Informe 2011-Observatorio Español de la Droga y las Toxicomanías: Situación y tendencias de los problemas de drogas en España.
- Encuesta Nacional de Salud de España, 2006. Available from: http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm
- Gomez-Pardo E, Fuster V et al. J Am Coll Cardiol, 2016, 67(5):476-85. A Comprehensive Lifestyle Peer Group-Based Intervention on Cardiovascular Risk Factors: The Randomized Controlled Fifty-Fifty Program.
- Glanz K and Bishop DB. Annu Rev Public Health, 2010, 31:399-418. The role of behavioral science theory in development and implementation of public health interventions.
- Karwalajtys T et al. J Community Health, 2009, 34(4):336-45. Development of the volunteer peer educator role in a community Cardiovascular Health Awareness Program (CHAP): a process evaluation in two communities.
- Thompson PD et al. Circulation, 2007, 115(17):2358-68. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology.
- Heath GW et al. Lancet, 2012, 380(9838):272-81. Evidence-based intervention in physical activity: lessons from around the world.
- Fernández-Alvira JM, Fuster V et al. Am Heart J, 2021, 240:81-88. The challenge of sustainability: Long-term results from the Fifty-Fifty peer group-based intervention in cardiovascular risk factors.
