COLOMBIA HEALTHY HABITS FOR LIFE PROGRAM
“IN 2009 WE EDUCATED AND FOLLOWED A SAMPLE OF 1.250 FROM 3 TO 7 YEARS OLD COLOMBIAN KIDS FOR THREE YEARS AND WE HAVE SEEN EVERYTHING WE EXPECTED. THIS IS AN IMPORTANT PROTOCOL, NOBODY HAS SOMETHING LIKE THIS. 650 STUDENTS HAVE GROWN UP TO 6 to 10 YEARS OLD AND RESEARCHERS NOW WORK TO DETERMINE HOW MUCH OF THE HEALTH EDUCATION THEY HAVE RETAINED SINCE 2009. THE PLAN IS TO FOLLOW THE SAMPLE UNTIL YEAR 2030. THE WINNER IN THIS PROJECT IS OBSESSIVENESS”

The Colombia Programme: Promoting healthy habits in children in order to prevent cardiovascular diseases
Unhealthy lifestyle habits can lead to the development of cardiovascular diseases. Recent data suggest that lifestyle habits are acquired at an early age, specifically at around 3-8 years of age, and persist into adult life. To provide further data on children, Dr. Fuster, in collaboration with the famous television shows “Sesame Street” and “Plaza Sesamo” designed a community intervention study in 14 Colombian schools. The aim of the programme targeted to children between 3-5 years





of age, their parents and teachers, was to promote the development of healthy habits that persist into adult life, through leisure-educational activities focusing on nutrition, a healthy heart and the importance of physical exercise. The initial results obtained appear to confirm that early educational interventions in school children significantly increase the knowledge which children have of their own body, and promote adoption of healthy habits over the long term.
Cardiovascular diseases are still the leading cause of death in the world [1]. These are complex diseases that are due to different risk factors, most of them modifiable, that are acquired in very young ages. Once the behaviors have been acquired, they continue in adulthood [2, 3]. The current society has developed environments that in most cases do not favor that individuals acquire and maintain healthy lifestyles. Experts agree that the only way to avoid the increase in cardiovascular diseases is a change in the lifestyle of the population and raising awareness of the need for promoting healthy lifestyles. With this regard, cardiovascular health promotion in children means a major
* Alliance between the Hospital Mount Sinai Heart, the Sesame Workshop in New York, US, and the Fundación Cardioinfantil (Foundation for the care of Children’s Heart) of Bogotá, Colombia
opportunity for primary prevention, in particular in emerging countries, where a significant change is taking place in health-related behaviors. [4]. The structure to implement these strategies should include school and community programs that promote physical activity and a heart-healthy diet, for the purpose of fighting the burden of chronic diseases associated with a sedentary lifestyle and obesity [5-8]. Based on the above, the SI Colombia Program performed a study in Colombia under the assumption that educational interventions starting at an early age can promote that healthy behaviors and attitudes are adopted later. Therefore, with the collaboration of the Fundación Julio Mario Santo Domingo and the famous TV program “Sesame Street”, in 2009 Dr. Fuster started up in Bogotá a program to educate pre-school children about subjects related to exercise, healthy diet and understanding of the body.
The study included 1,216 children aged 3 to 5 years, 928 parents, and 120 teachers from 14 schools. The participating schools were randomly divided into two groups (1:1). Seven schools were part of the intervention group for cardiovascular health promotion, while the other 7 schools were the control group, i.e., no intervention was performed in them (only a follow-up during the same time period to compare the results, though, once the study was ended, the students of these schools did receive a similar training [9]) (Figure 1).
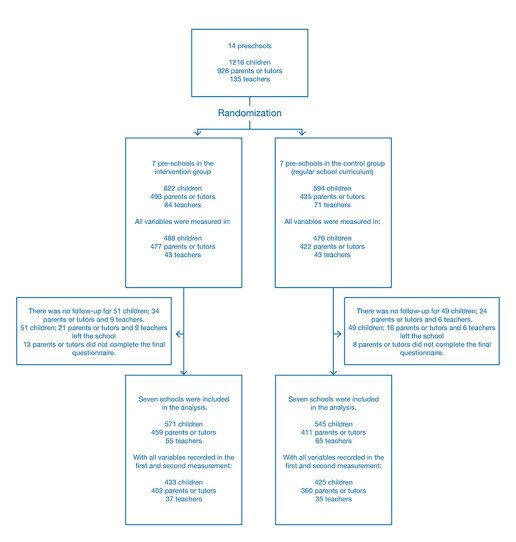
Figure 1. Enrollment, randomization and follow-up of the study population.
The children included in the intervention group received one daily hour of training on healthy lifestyles and on the function of the human body. Education was given by teachers (previously trained with the support of a guide with the materials of “Sesame Street”) using videos and board games (“heart game”), as well as through tales, songs and placing posters in classrooms with subjects related to health [9]. In addition, both children and parents and teachers participated in workshops lasting one hour a week (“Day of the healthy family”), where printed information was handed out about how to promote physical exercise or improve diet [9]. Parents were also given 3 workshops focused on promoting the consumption of healthy food and practicing sports. For instance, in areas with a poor access to parks or recreational facilities, the parents were trained to encourage their children to use stairs instead of elevators and to walk instead of taking the bus [9].
To evaluate objectively the effect of the intervention, the investigators used questionnaires to measure both in children (primary study objective) and in parents and teachers (secondary objective) the level of knowledge of the body and the heart, the physical activity level and the healthy diet habits and lifestyle. The measurements were performed before starting the intervention and at 6 and 18 months of starting it. The questionnaires were developed by psychologists, pediatricians, educators and experts in children nutrition and development. The weight and height of children were also measured at the study start, just at the end of the intervention and one year after the end of the program.
At the end of the intervention, the investigators documented a greater increase in the total score on the knowledge, attitude and healthy lifestyles in children participating in leisure-educational activities (+10.9%) as compared to children in the group not receiving this training (+5.3%). This increase was also greater in parents and teachers from the intervention group (+8.9% and + 9.4%) than in parents and teachers from the control group (+3.1% and +2.5%, respectively). In addition, in the intervention group this improvement in the knowledge and acquisition of healthy habits persisted in all cases after one year of ending the program [9].
After 3 years, the investigators evaluated again 598 children and 475 parents participating in the study. With regard to the time when the study was performed, an improvement of 15% was seen in the knowledge of the children, of 51% in their attitude towards the matter, and of 27% in their healthy lifestyles. In addition, the percentage of children with an adequate weight increased from 62% to 75% [10].
+In 2017, assuming that the effects of the pedagogical intervention can decrease over time, a new follow-up is underway for the purpose of establishing, in a first stage, the differences in a baseline measurement in terms of knowledge, attitudes, habits and emotions (KAHE) of children aged from 10 to 13 years of the Usaquén cohort and a comparable cohort in Bogotá (n = 1,200) and in the cardiovascular health of children and parents from both cohorts. Therefore, the towns where they live and the schools of the children of the Usaquén cohort were identified. 650 children/families of the 1,216 belonging to the original cohort, 530 (81.5%) from the towns of Usaquén and Suba, in private and public schools (n = 70 schools). Therefore, the towns where they live and the schools of the children of the Usaquén cohort were identified.
The information to date for this field is:
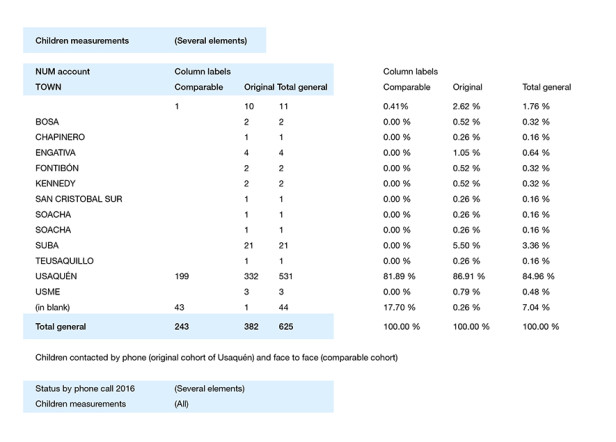
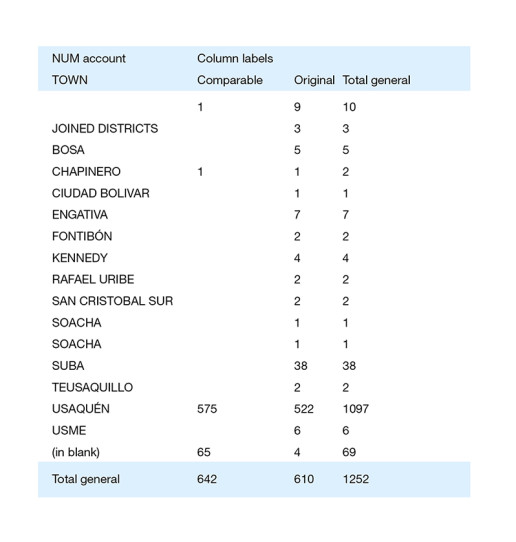
For the comparable cohort, children from schools distributed proportionally in the towns where the children of the Usaquén cohort live were selected for the purpose of having a population as comparable as possible in terms of age, social-economic level and sex. The study candidates were contacted by phone to be invited to an informative meeting (August 2016). During the months of September and October 2016, cardiovascular health was measured in children and adults (Table 1) and KAHE in children.[11] The data collected will be recorded in an Excel database, 2010 version, and a statistical analysis will be performed. The prevalence (95% CI) of each of the 7 components of cardiovascular health rated as poor (risk factor) will be measured and the differences between these prevalences and between these means of the scores and the standard deviations of KAHE to a healthy lifestyle will be evaluated at the start of the study in both groups (Usaquén cohort and comparable cohort).
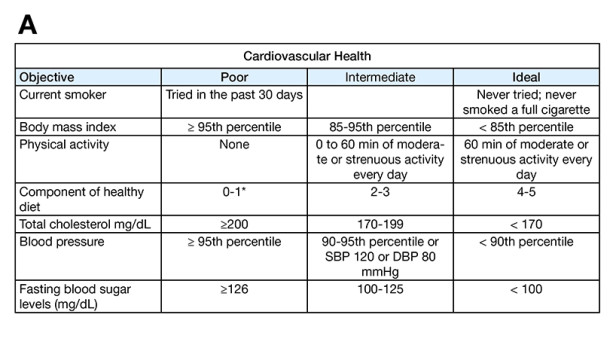
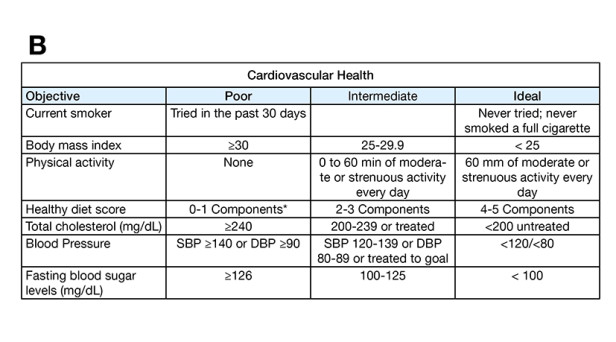
Table 1. Definitions of cardiovascular health in children (A) and in adults older than 20 years (B) according to the American Heart Association. *Fruits and vegetables: ≥ 4.5 cups a day; fish: ≥ two portions of 3.5-oz a week (preferably fatty fish); whole grains rich in fiber (≥ 1.1 g of fiber per 10 g of carbohydrates): ≥ three portions of 1 oz, per day; sodium: < 1500 mg a day;* drinks sweetened with sugar: ≤ 450 kcal (36 oz) per week.
In a second phase, the impact of a four-month educational community intervention (given in the community centers of the Zone Planning Units (ZPU) of the towns of Usaquén and Suba) (Table 2) in the cardiovascular health and KAHE to a healthy lifestyle of children from these cohorts will be evaluated through a randomized, controlled trial (Figure 2). The group subject to intervention will include 600 boys and girls, some of them selected at random from those participating in the first study (2009). There will be a control group with 600 children also to work with them around performing school work.
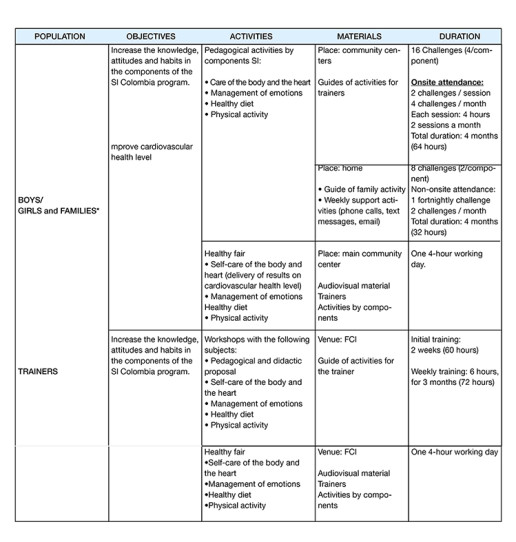
Figure 2. Clinical trial flow chart. CHI: Cardiovascular Health Index, KAHE: Knowledge, attitudes, habits, emotions.
Table 2. Components of the educational and community intervention. *The intervention is aimed at children. Parents / care givers will be given: a guide and the challenges selected (activities) to be developed at home; phone calls, texts and e-mails to remind and motivate families to fulfill these activities with their children; short informative sessions (45 minutes) in each face-to-face session; and the invitation to a motivational and information event.
At each community center (a total of 6, each with two rooms prepared) there will be 3-hour working days, one Saturday every eight days (intervention group one Saturday and control group next Saturday, so that each group will meet every 15 days). The working days will take place on Saturdays in the morning and in the afternoon. Each day will include working with 25 different children in the 12 rooms available.
As in phase 1, the data (Table 3) will be recorded in an Excel database, 2010 version, and a statistical analysis will be performed. The effect of the intervention will be calculated with the same method used in the first phase.
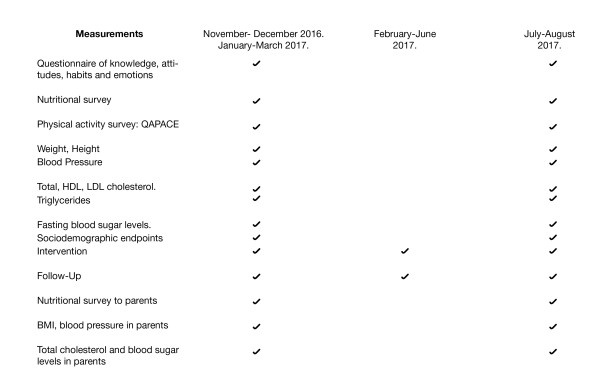
Table 3. Gathering information.
In conclusion, the study has shown that dedicating forty hours of training preschool children in healthy habits significantly increases the knowledge they have of their own bodies, as well as effectively promotes the adoption of these habits. These improvements have continued to be seen three years after the intervention, when the children were already between six and eight years old, a fact that demonstrates that the benefits of an educational program of these characteristics are maintained in the long term [10]. However, a re-intervention was made 7 years later to 596 children between 9 and 13 years old from the first study, and compared with a group of 620 children of the same age who had not been intervened in the preschool stage. No statistically significant differences were found between the groups after the intervention at 9-13 years old, so it seems important that re-intervention strategies are carried out at an earlier age to maintain a sustained effect of the preschool intervention [12].
References
- Adeyi O, Smith O. and Robles S. World Bank Publications, Washington, DC. 2007. Public policy and the challenge of chronic noncommunicable diseases.
- Deshmukh-Taskar P et al. Eur J Clin Nutr, 2006, 60(1):48-57. Tracking of overweight status from childhood to young adulthood: the Bogalusa Heart Study.
- Freedman DS et al. Pediatrics, 2001, 108(3):712-8. Relationship of childhood obesity to coronary heart disease risk factors in adulthood: the Bogalusa Heart Study.
- World Health Organization (WHO). Global Strategy on Diet, Physical Activity and Health.
- Centers for Disease Control and Prevention, Coordinating Center for Health Promotion. 2008. Physical Activity and Good Nutrition: Essential Elements to Prevent Chronic Diseases and Obesity.
- Summerbell CD et al. Cochrane Database Syst Rev, 2005(3):CD001871. Interventions for preventing obesity in children.
- Ekelund U et al. JAMA, 2012, 307(7):704-12. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents.
- Task Force on Community Preventive Services. MMWR Recomm Rep. 2001, 50(RR-18):1-14. Increasing physical activity: a report on recommendations of the Task Force on Community Preventive Services.
- Céspedes J, Fuster V et al. Am J Med, 2013, 126(1):27-35 e3. Targeting preschool children to promote cardiovascular health: cluster randomized trial.
- Céspedes J, Fuster V et al. Am J Med, 2013, 126(12):1122-6. Promotion of cardiovascular health in preschool children: 36-month cohort follow-up.
- Donald M et al. Circulation,2010, 121:586-613. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond.
- Fernández-Jiménez R, Fuster V et al. J Am Coll Cardiol, 2020, 75:13. Sustainability of and adherence to preschool health promotion among children 9 to 13 years old.
